
“The acquisition of healthy habits from childhood reduces the risk of cardiovascular diseases and improves the quality of life in adulthood”
DR. VALENTÍN FUSTER
“The acquisition of healthy habits from childhood reduces the risk of cardiovascular diseases and improves the quality of life in adulthood.”
DR. VALENTÍN FUSTER
SI! Program
Hypothesis
The acquisition of healthy habits from childhood reduces the risk of cardiovascular diseases and improves the quality of life in adulthood.
The main cardiovascular risk factor, in both adults and children, is obesity and its associated conditions (diabetes and arterial hypertension), resulting from poor eating habits and a low level of physical activity [1]. The epidemiological data indicate that cardiovascular risk factors are present from increasingly on early ages, and that the poor eating habits acquired in childhood persist on into adult life [2-6]
In addition, other cardiovascular risk factors such as alcohol abuse, smoking and the use of other drugs are also beginning to manifest in the Spanish (pre)-adolescent population [7,8]. Public health research has shown that health-promoting initiatives should start in childhood in order to secure lasting and effective behavioral changes. [9-12].
The SI! Program consists of an intervention in educational centres to promote cardiovascular health from the pre-school stage. Its aim is to demonstrate that the acquisition of healthy habits from childhood reduces the risks of cardiovascular disease and improves quality of life in adulthood.
The SI! Program consists of four basic, interrelated components:
- Acquisition of Healthy eating habits
- Active living
- Knowledge of the body and heart
- Management of emotions

Promoting
healthy eating
Promoting
active lifestyle
Knowledge of the body and the heart
Learn how to manage emotions
Figure 1. Components and levels of intervention SI! Program
The program operates at four levels: school environment, teachers, families and pupils.
The intervention at the school environment level is carried out through strategies that involve the entire educational community, including families.
The action at the teacher level aims, on the one hand, to make the teaching staff aware of the reality of cardiovascular disease and the importance of their contribution as educators in the acquisition of healthy habits in the school population and, on the other hand, to train teachers in healthy habits and in the methodology to be followed to teach the program in the classroom and provide them with materials and tools to work with students. This training course is accredited by the different Autonomous Administrations.
The contents of the program were checked by educational psychologists and teachers at the centres, as well as being in line with the school curriculum. Special emphasis is placed on their involvement in order to achieve changes in routines and habits in the family environment [13].
The SHE Foundation has carried out several scientific studies in different Educational Stages to demonstrate the hypothesis of the SI! Program.
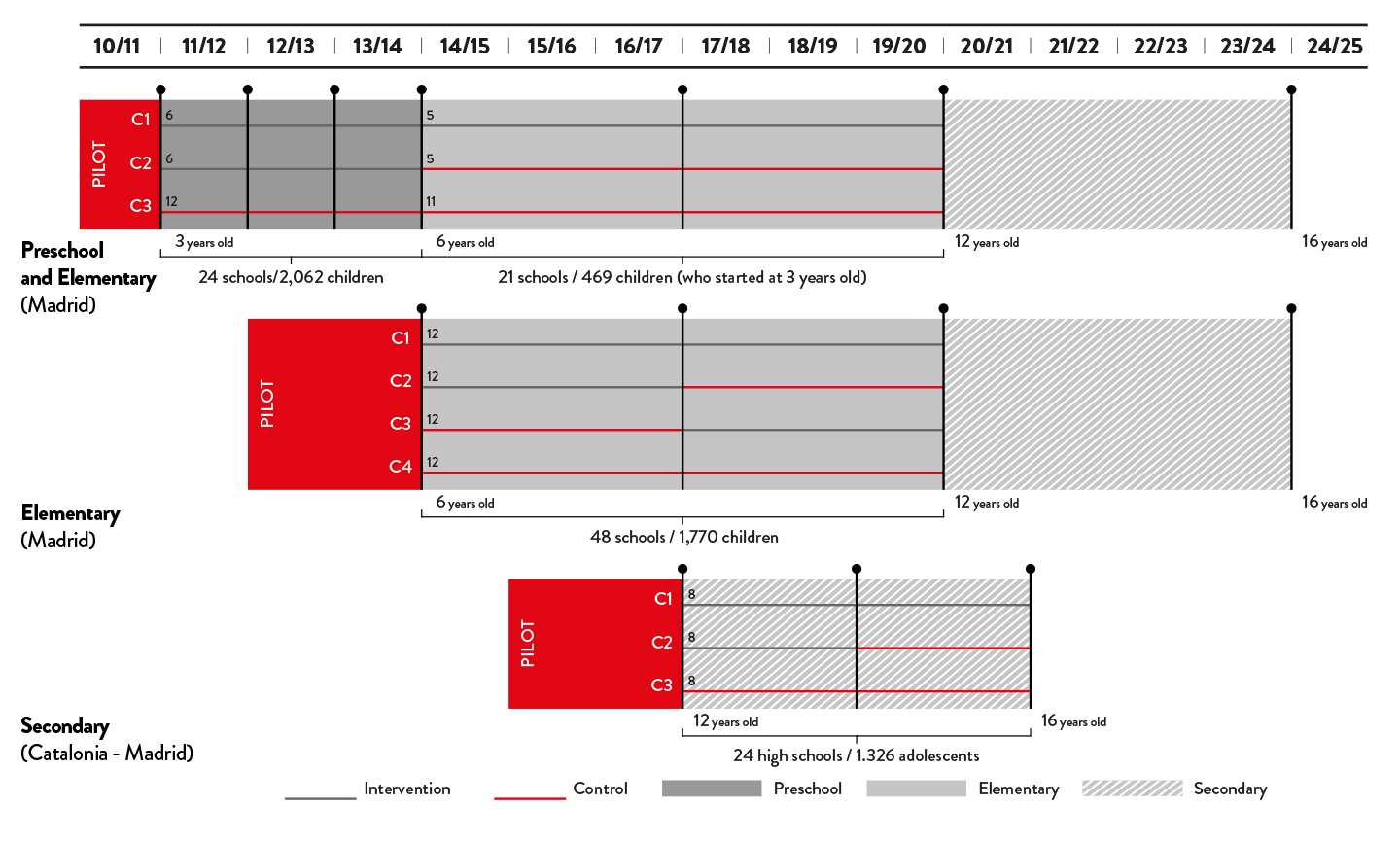
Figure 2. Scientific studies of the SI! Program in Preschool, Elementary and Secondary
Infant Education Stage
This was carried out from 2011 to 2014 in 24 state schools in Madrid through a randomised, controlled study. Half of the schools that participated in the study were randomly assigned to the intervention group, whose students carried out a minimum of 30 hours of activities per academic year focusing on the program components on emotion management, additional weekend activities with family members, annual health fairs, etc. Students in the remaining (control) schools continued with their usual curriculum [13].
A dozen researchers from the National Centre for Cardiovascular Research and Mount Sinai Hospital evaluated the effectiveness of the SI! Program in 2,062 children aged 3-5 years. The results of the study showed that the implementation of the program led to a significant increase in children’s knowledge, attitudes and healthy habits, as well as an improvement in markers of adiposity [13].
In conclusion, the SI! Program contributes new and valuable information on the benefits of an early intervention targeted to pre-school children, referred to the promotion of healthy life habits. According to Dr. Fuster, “the basis of the program is the fact that it is between 3-6 years of age when we develop our future behavior as adults. Cardiovascular disease has a lot to do with behavior, and so here we have our window of opportunity”.
This study moreover uses an innovating design, since it expands the role of physicians to also encompass the teaching community. On the other hand, it involves a protocol with structured evaluation, something that is usually lacking in community public health interventions. The program moreover coordinates families and educators through the pupils, which may serve to guarantee the sustainability of the intervention.
Currently, the SI! Program has been extended to more than 125 schools in the Community of Madrid, Catalonia and Galicia.
Primary Education Stage
In Madrid, a randomized study was carried out from 2014 to 2020 in the primary education stage (children aged 6 to 11 years). Forty-eight public schools from 16 municipalities in the south of Madrid participated, with a total of 1,770 children, their families and teachers [14]. A randomization was carried out in 4 groups of schools with different exposure to the SI! Program. The aim of this design was to evaluate the effect of the SI! Program at different times and with different intensities. Additionally, the children participating in the randomized study of the SI! Program were followed up. In this way, it will be possible to evaluate the effect of the SI! Program in the long term and with different intensity of exposure to the intervention.
Although the final study measurements were taken during the lockdown caused by the COVID-19 pandemic, the results show a beneficial effect of the SI! Program on indicators of adiposity and body weight, especially for those benefitting from the implementation of the program in the early years of the primary school [15].
The results obtained from all SI! studies have shown that the effect of the intervention on children’s health is likely to be more sustainable if it is started as early as possible and includes reinterventions to reinforce key messages to families until children become more independent.
Through a new randomised study starting in the 2023-24 school year in Madrid, a primary school version of the SI! Program will be implemented using all the experience gained over the last ten years, which has led to the design of a reintervention strategy in the classroom and a reinforcement of actions at school and family level.
At the same time, the study will be carried out in the town of Mataró, located near Barcelona, , where the SI! Program It has been implemented since 2012.
This marks Mataró’s first participation in a randomized study, enabling a comparison and consolidation of results from both locations.
Secondary Education Stage
SI! Program has been applied in Secondary Education through a randomized design from 2017 to 2021. The project, awarded by the Marató of TV3 in collaboration with the University of Barcelona, the National Center for Cardiovascular Research and SHE, has included 1,326 adolescents aged 12 to 16 years from 24 public high schools in the north of Madrid, Barcelona and Baix Llobregat [16]. Most early adolescents enrolled in the SI! Program for Secondary School trial had a poor or intermediate cardiovascular health at baseline, with just 11% of them demonstrating ideal cardiovascular health [17]. The lowest scoring individual component was dietary habits, with only 0.6% of adolescents meeting ideal recommendations.
The SI! Program was implemented in at least the first two years of secondary school, and the results show that the distribution of content throughout the entire Stage led to greater cardiovascular health benefits for adolescents compared to those experienced with the intensive implementation of content during the first two years of the Stage [18].
Although the COVID-19 pandemic did not allow the full potential of the intervention to be evaluated, these results confirm that the effect of school-based interventions promoting health are influenced by factors such as the duration and magnitude of the content delivered.
References
- Caballero B. Epidemiol Rev, 2007, 29:1-5. The global epidemic of obesity: an overview.
- Fuster V and Kelly BB. Washington, DC: National Academies Press, 2010. Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health.
- Carlsson AC et al. Int J Cardiol, 2013, 168(2):946-52. Seven modifiable lifestyle factors predict reduced risk for ischemic cardiovascular disease and all-cause mortality regardless of body mass index: a cohort study.
- Rodriguez-Artalejo F et al. Eur J Clin Nutr, 2002, 56(2):141-8. Dietary patterns among children aged 6-7 y in four Spanish cities with widely differing cardiovascular mortality.
- Roman B et al. Nutr Rev, 2009, 67 Suppl 1:S94-8. Physical activity in children and youth in Spain: future actions for obesity prevention.
- Martinez-Vizcaino V et al. Public Health Nutr, 2009, 12(7):1015-8. Trends in excess weight and thinness among Spanish schoolchildren in the period 1992-2004: the Cuenca study.
- Garces C and de Oya M. Rev Esp Cardiol, 2007, 60(5):517-24. [Cardiovascular risk factors in children. Main findings of the Four Provinces study].
- Martinez Vizcaino V et al. Med Clin (Barc), 2006, 126(18):681-5. [Prevalence of obesity and trends in cardiovascular risk factors among Spanish school children, 1992-2004: the Cuenca (Spain) study].
- Gubbels JS et al. Int J Behav Nutr Phys Act, 2012, 9:77. Clustering of energy balance-related behaviors in 5-year-old children: lifestyle patterns and their longitudinal association with weight status development in early childhood.
- Mishra S et al. J Basic Clin Physiol Pharmacol, 2013, 18:1-8. Association of diet and anthropometric measures as cardiovascular modifiable risk factors in young adults.
- Story M. Int J Obes Relat Metab Disord, 1999, 23 Suppl 2:S43-51. School-based approaches for preventing and treating obesity.
- Williams CL et al. Circulation, 2002, 106(1):143-60. Cardiovascular health in childhood: A statement for health professionals from the Committee on Atherosclerosis, Hypertension, and Obesity in the Young (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart Association.
- Peñalvo JL, Fuster V et al. J Am Coll Cardiol, 2015, 66 (14):1525-1534.The SI! Program for cardiovascular health promotion in early childhood: A cluster randomized trial.
- Santos-Beneit G, Fuster V et al. Am. Heart J, 2019, 210:9-17. Rationale and Design of the SI! Program for Health Promotion in Elementary Students Aged 6 to 11 years: A Cluster Randomized Trial.
- Santos-Beneit G, Bodega P, de Cos-Gandoy, A et al. J Am Coll Cardiol. 2024; 84(6):499-508. Effect of Time-Varying Exposure to School-Based Health Promotion on Adiposity in Childhood.
- Fernández-Jiménez R, Fuster V et al. Am. Heart J, 2019, 215:27-40. Rationale and design of the school-based Program SI! To face obesity and promote health among Spanish adolescents: a cluster-randomized controlled trial.
- Fernández-Jiménez R, Fuster V et al. Eur. J. Prev. Cardiol, 2020, doi:10.1093/eurjpc/zwaa096. Prevalence and correlates of cardiovascular health among early adolescents enrolled in the SI! Program in Spain: a cross-sectional analysis.
- Santos-Beneit G, Fernández-Alvira JM, Tresserra-Rimbau A et al. JAMA Cardiol. 2023;8(9):816-824. School-Based Cardiovascular Health Promotion in Adolescents: A Cluster Randomized Clinical Trial.

All rights reserved. The total or partial reproduction of this work is not allowed. You may not copy, reproduce, distribute, publish, display, perform, modify, create derivative works, transmit, or in any way exploit any such content, nor may you distribute any part of this content over any network, including a local area network, sell or offer it for sale, or use such content to construct any kind of database without prior written authorization from the owners of the work copyright. The infringement of said rights may constitute a crime against intellectual property.
